I Had an 85-Degree Scoliosis Curve
The surgeon reached for his hardware catalog. I said no.



I was eighteen. The X-ray showed an 85-degree S-curve. The kind of number that ends conversations. At that degree, the clinical pathway narrows to one option: metal rods, fusion, a spine that will be straighter but will never bend the same way again.
He described the procedure. I listened. I understood. And something in me refused. Not from knowledge. I did not have a plan. I did not have an alternative. I just knew, in a way I could not articulate at eighteen, that fusing my spine was not the answer. That the curve was not the whole problem. That something underneath it was being missed.
I would not understand what that something was for another fifteen years.
Can scoliosis be fixed in adults?
It depends on what you mean by “fixed.”
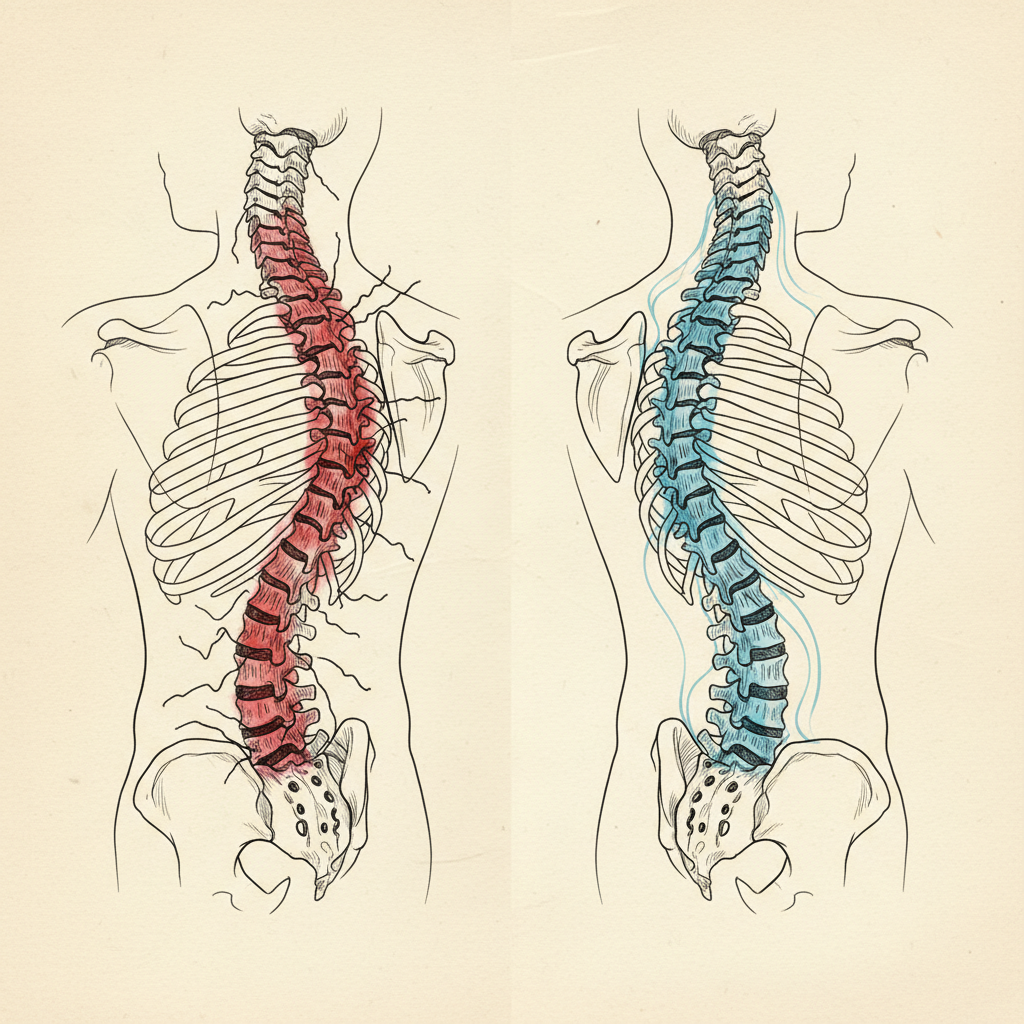
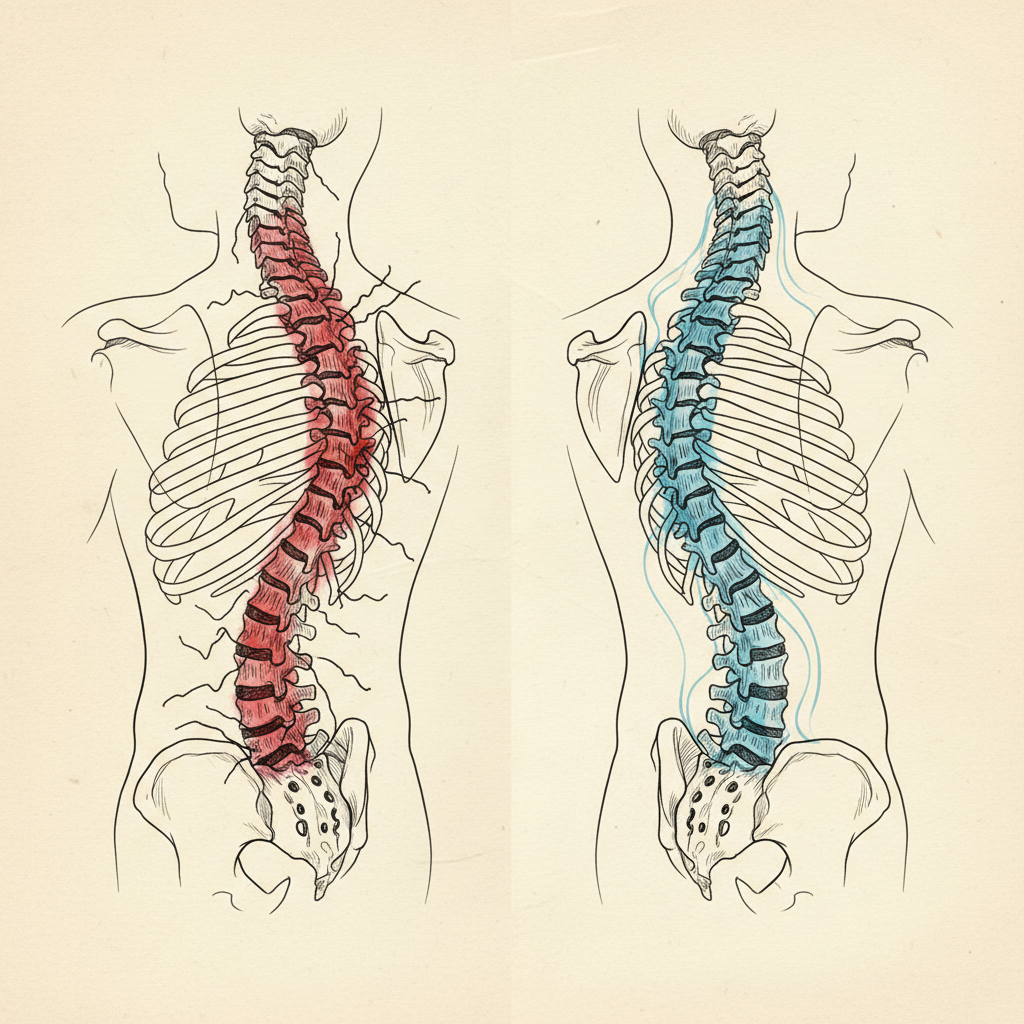
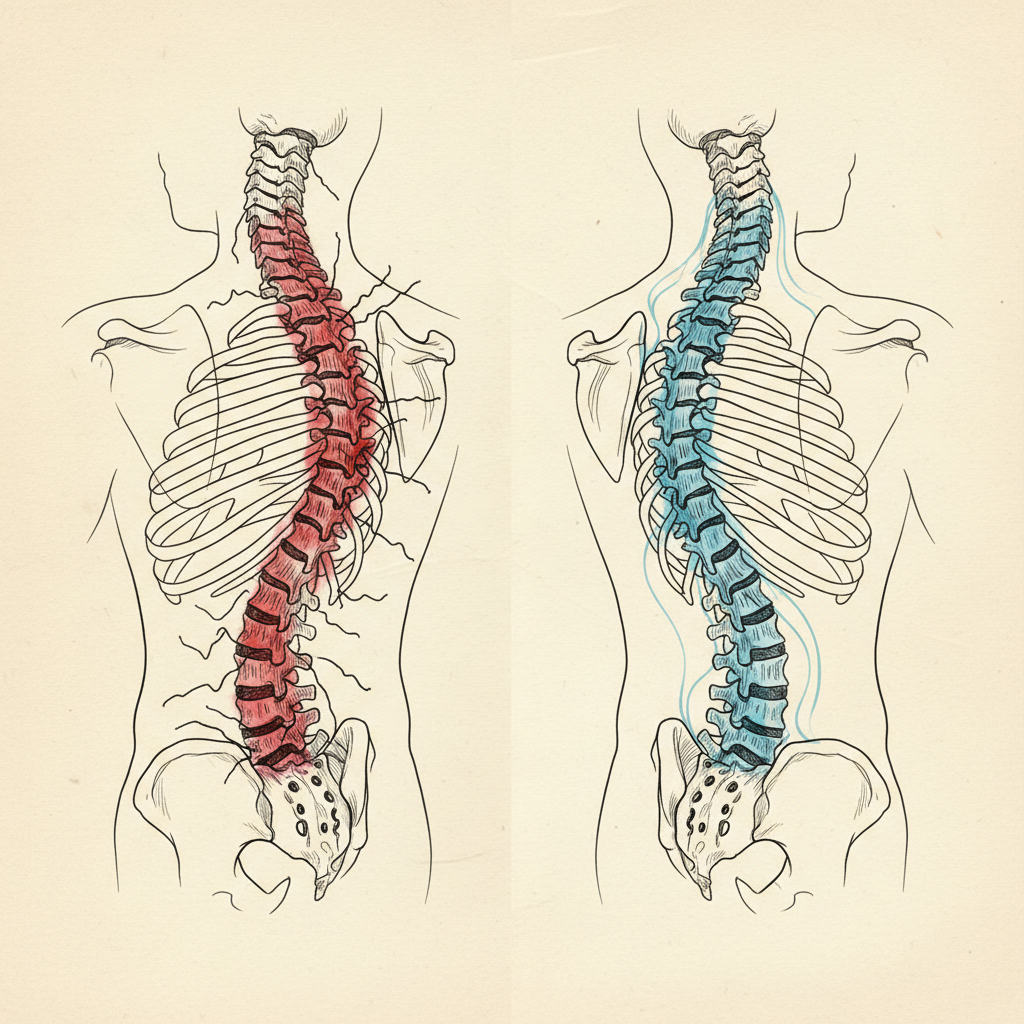
Scoliosis in adults cannot be reversed to a perfectly straight spine. The structural bone changes from years of asymmetric loading are real. But the bracing pattern that maintains the curve, the pressure asymmetry that drives it, and the body schema distortion that reinforces it are all neurological, not structural. These can change at any age.
The curve may not disappear. But the forces maintaining it can be reorganized. Pain can resolve. Function can return. Height can increase. The body can find a new equilibrium that is dramatically different from the old one.
I know this because it happened to me. Two inches of height gained, without surgery, without a brace, without anyone touching my spine. Two inches that came from updating what my nervous system believed was true about my body.
But that is the end of the story. Let me tell you the middle.
Fifteen years of the wrong model
From eighteen to thirty-three, I tried everything the conventional model offered. Physical therapy. Chiropractic adjustments. Exercise protocols. Stretching routines. Some helped for a day. Some for two. Then my body returned to exactly where it had been.


Every approach shared the same assumption. That my spine was the problem. That the curve was a structural defect. That the solution was to move bones, stretch muscles, strengthen the weak side.
The curve did not respond. Because the curve was not the problem. The curve was the output. The printout. The visible expression of something happening deeper than any exercise could reach.
The shutdown
At thirty-three, my body collapsed. Not the spine. Everything.
Fatigue. Digestive shutdown. Systems going offline one by one. The curve was not just a cosmetic issue anymore. My life force was getting choked out.
I stopped working as normal. For eight months. Not a sabbatical. A desperation phase. I went looking with an intensity I had never brought before. Not for another exercise. Not for another practitioner. For the thing that everyone was missing.
Three discoveries
The first: posture is a prediction, not a position. My nervous system was not failing to hold my spine straight. It was actively organizing my spine into a curve. On purpose. Based on the sensory data it was receiving and the threat history it was carrying. The curve was not a defect. It was a strategy.
The second: the spine is a printout. The bones do not decide where to go. They go where the forces acting on them dictate. Those forces are pressure from the diaphragm, tension from the fascia, and instructions from the body schema. The bones are the output. The nervous system is the input.
The third: the diaphragm was the key. In my body, the diaphragm was mechanically distorted by the rotational component of the curve. It was generating pressure asymmetrically. One side of my abdominal canister was over-pressurized. The other side was deflated. The spine was deforming in the direction of pressure loss. And the fascia on the compressed side was over-tensioning to compensate. Not because it was “tight.” Because the pressure system underneath it had collapsed.
Changing the inputs
I did not stretch my way out of the curve. I did not strengthen my way out. I did not get adjusted out of it.
I changed the inputs.
I addressed the nervous system’s threat level. The bracing pattern that had locked my body for fifteen years was not muscular. It was autonomic. My nervous system was in a chronic state of protection. Until that state shifted, nothing else could change.
I rebuilt sensory resolution. I learned to feel the asymmetry. The pressure differential between left and right. The restriction in the diaphragm. The places where the body map had gone dark. I was not learning new movements. I was re-learning how to feel my own body.
I restored pressure symmetry. I learned to breathe in a way that pressurized the abdominal canister evenly. The diaphragm descended. The pelvic floor engaged. The sealed chamber that had been leaking for decades finally held pressure. And the surface muscles that had been gripping to compensate began to release.
I integrated into movement. Contralateral patterns. Spiral loading. Rotational intelligence. The new pressure organization had to hold under real-world demand, not just on a mat in a quiet room.
The body did not change overnight. It changed over months. Then years. But the direction was consistent. A sustained reorganization that accumulated because the model had updated, not just the position.
What the conventional model cannot explain
Under the mechanical model, what happened to me is not possible. An 85-degree curve in a skeletally mature adult is permanent. The growth plates are closed. The only intervention is surgical fusion.
Two inches of height. Measurable change. No surgery.
The conventional model cannot explain it because it assumes the bones are the problem. The bones are the printout. The nervous system is the printer. When you change what the system prints, the structure reorganizes. Not to a straight spine. But to a dramatically different equilibrium where the forces maintaining the curve have been renegotiated.
What this means for you
If you have scoliosis as an adult, you have been told a story. The story says your spine is defective, the curve is permanent, management is the best you can hope for.
The structural changes are real. The bone remodeling is real. A mature spine does not straighten like an adolescent spine under a brace.
But the story is incomplete. It leaves out the nervous system. It leaves out the body schema. It leaves out the pressure mechanics that maintain the curve long after the structural changes have set. It leaves out the fact that the bracing pattern is neurological, not structural, and neurological patterns can change at any age.
Yola, one of our cohort participants, is 67 years old with an 84-85 degree S-curve. Week two of the program, she described what happened when she found organized pressure: “I didn’t have to stay straight or feel the twist. I didn’t have to do any work. It just worked.”
Sixty-seven. A curve nearly identical to mine. “It just worked.”
Your nervous system organized the best structure it could with the signals it was receiving. Change the signals, and the body reorganizes. I sat in that surgeon’s office at eighteen and said no without knowing why. It took fifteen more years to find the reason. The spine is a printout. And you do not fix a printout by cutting it. You fix it by changing what the system believes is true.
Sources
- Friston, K. (2010). The free-energy principle: a unified brain theory? Nature Reviews Neuroscience, 11(2), 127-138. [T1]
Posture as prediction. The nervous system actively organizes the curve, not passively holding it. - Paillard, J. (1999). Body Schema and Body Image: A Double Dissociation in Deafferented Patients. In G.N. Gantchev et al. (Eds.), Motor Control, Today and Tomorrow. [T1]
Body schema as the internal map generating postural output. Updating the schema changes the output. - Kolar, P., et al. (2012). Postural function of the diaphragm in persons with and without chronic low back pain. Journal of Orthopaedic & Sports Physical Therapy, 42(4), 352-362. [T1]
Diaphragm as postural stabilizer. IAP as the internal scaffolding system. Pressure asymmetry driving spinal deformation. - Langevin, H.M., et al. (2011). Reduced thoracolumbar fascia shear strain in human chronic low back pain. BMC Musculoskeletal Disorders, 12, 203. [T1]
Fascial remodeling along lines of chronic loading. Structural adaptation to sustained compensatory forces.
Leave a Reply